Did you know that nocturnal hypokinesia affects nearly 70% of individuals living with Parkinson’s disease, making simple tasks like turning over in bed a major physical challenge? This condition manifests as a marked reduction in the amplitude and frequency of voluntary movements, often causing people to feel as though their muscles are restricted without a direct loss of strength. When gestures like swinging the arms or changing facial expressions begin to fade, it signals a disruption in the brain’s motor circuits or, in some cases, a weakening of the cardiac muscle.
Distinguishing between neurological and cardiac origins is vital for selecting the correct treatment path. This article explores the clinical markers of reduced movement and provides a clear overview of the management strategies available to help restore motor function and daily independence.
- Understanding Hypokinesia in Clinical Practice
- Common Motor Symptoms and Physical Markers
- Pathophysiology of the Basal Ganglia Loop
- Primary Causes and Parkinsonian Syndromes
- Therapeutic Interventions and Management Options
- Prognosis and Complicating Lifestyle Factors
Understanding Hypokinesia in Clinical Practice
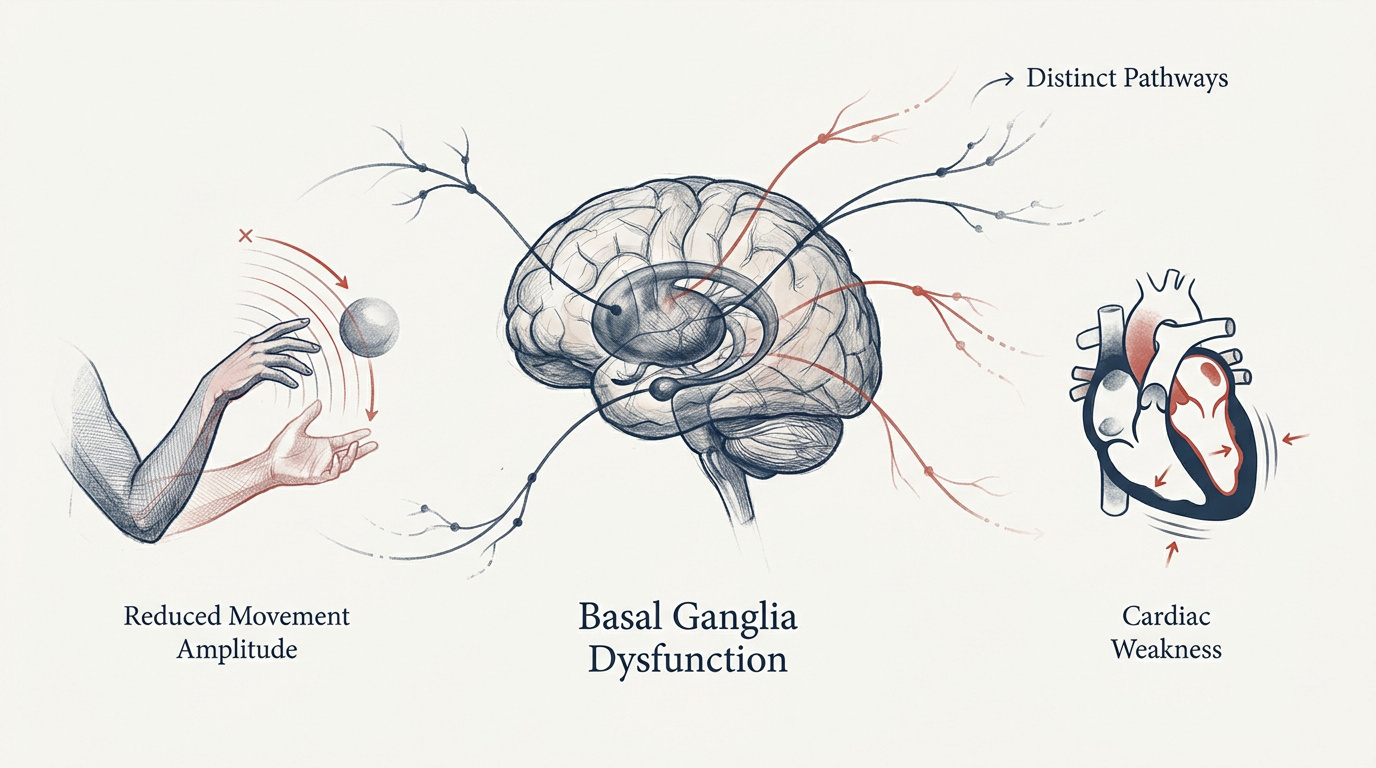
Hypokinesia involves reduced movement amplitude or speed, often signaling basal ganglia dysfunction. While neurological cases relate to Parkinson’s, cardiac hypokinesia affects ventricular wall motion, requiring distinct diagnostic pathways for effective motor or heart management.
The physical manifestation of this condition starts with a noticeable decrease in the range of voluntary actions.
Hypokinesia is a reduction in movement amplitude or frequency without loss of motor strength, unlike paralysis. Examples: reduced frequency of crossing legs or folding arms.
Reduced Amplitude Versus Speed of Movement
Hypokinesia is defined as a specific reduction in the range of motion. It differs from simple weakness. The brain struggles to scale movements correctly.
Daily tasks like reaching for a cup become difficult. The physical execution lacks the necessary breadth. Muscles aren’t paralyzed but restricted. This affects all voluntary motor functions significantly.
Normal motor function disappears. Simple gestures feel heavy and small.
Distinction Between Akinesia and Bradykinesia
Akinesia represents the total inability to initiate movement. Bradykinesia refers to the slowness of execution.
Clinical boundaries are often blurred in practice. However, precise terminology is vital. It helps pinpoint the exact stage of neurodegeneration.
Modern research highlights the evolution of the medical terminology. This ensures more accurate diagnostic frameworks.
Neurological Versus Cardiac Manifestations
Cardiac hypokinesia describes a weak heart muscle contraction. It specifically affects the left ventricular wall. This is entirely separate from brain-related motor issues. Doctors must clarify this distinction early.
Involves ventricular wall motion and chronic heart failure risks.
Relates to basal ganglia circuits and conditions like Parkinson’s.
Patients often confuse heart health with brain health. Cardiology and neurology involve very different specialties. Misunderstanding the term can lead to unnecessary anxiety.
Diagnostic paths differ. One focuses on blood, the other on nerves.
Common Motor Symptoms and Physical Markers
Beyond the technical definitions, hypokinesia manifests through visible physical markers that alter a person’s daily presence.
Facial Expression and Fine Motor Skills
Hypomimia creates a “masked face” appearance. Emotional expressions become muted and slow. This often leads to social misunderstandings and isolation.
Fine motor skills deteriorate noticeably over time. Handwriting becomes tiny and cramped, known as micrographia. Buttons and zippers become major obstacles. These changes reflect the loss of precise control.
Non-verbal communication suffers deeply. People might seem disinterested or angry. It is purely a physical restriction of facial muscles.
Gait Patterns and Postural Changes
The characteristic shuffling walk is a major red flag. Steps become short and feet barely leave the ground. Arm swing is often absent on one side. This gait is highly inefficient.
Posture shifts forward into a stooped position. The center of gravity becomes unstable. Balance is compromised during even simple turns.
Motor instability increases the risk of dangerous falls. Freezing of gait can occur in narrow spaces. Constant vigilance is required for safety.
Risk of falls increases due to shuffling gait and loss of balance. Note the difficulty of turning in bed (nocturnal hypokinesia) affecting 70% of Parkinson’s patients.
Muscle Rigidity and Nocturnal Impact
Rigidity feels like constant stiffness in the limbs. Muscles resist passive movement throughout the day. This creates a heavy, leaden feeling for the patient.
Nocturnal hypokinesia is a particularly distressing symptom. Patients struggle to turn over in bed at night. This significantly disrupts sleep quality for many. It affects nearly 70% of those with Parkinson’s.
This lack of mobility during rest leads to significant fatigue. Poor sleep patterns further aggravate daily motor performance. You can read more about the impact of nocturnal hypokinesia on sleep to understand these systemic effects.
Pathophysiology of the Basal Ganglia Loop
Understanding these physical symptoms requires a look at the complex neural circuits governing our every move.
Dysfunction in the Thalamocortical Circuit
The brain uses a complex loop for signaling. The thalamocortical circuit acts as the primary highway. It connects motor planning with actual muscle execution. Disruptions here lead directly to motor inhibition.
The basal ganglia act as a gatekeeper. They filter out unwanted movements. When they fail, the “go” signal is suppressed.
This failure results in the characteristic slowness. The motor cortex receives insufficient stimulation. Voluntary actions become difficult to produce.
Neurotransmitter Roles of Dopamine and GABA
Dopamine depletion is the core chemical issue. It occurs within the substantia nigra. Without it, the motor circuit loses its balance.
Research indicates that hypokinesia stems from the perte des cellules dopaminergiques et l’hyperactivité de la voie indirecte. This disruption creates a persistent brake on movement. The system fails to initiate motor commands effectively.
GABA plays a massive inhibitory role here. It overpowers the signals needed for movement. This chemical imbalance stops smooth motor flow.
Impact of Glutamate on Motor Control
Glutamate provides excitatory influence on the subthalamic nucleus. Overactivity in this pathway causes further suppression. It creates a “braking” effect on movement.
These chemical shifts are not just abstract. They correlate directly with observable clinical symptoms. Doctors use this knowledge to target specific treatments. Balancing these neurotransmitters is a delicate task.
Too much glutamate can be toxic. It worsens the underlying neurodegeneration over time. Managing this is vital for long-term health.
Primary Causes and Parkinsonian Syndromes
While the chemistry is universal, the underlying causes of hypokinesia vary significantly between different medical conditions.
Differentiating Parkinson-plus From Primary Disease
Multiple System Atrophy presents unique challenges. Progressive Supranuclear Palsy also mimics standard Parkinson’s. These are known as ““Parkinson-plus” syndromes. They often involve more rapid clinical decline.

Standard treatments like levodopa often fail. The brain damage is more widespread. Specific markers help specialists identify these cases.
Early diagnosis changes the management plan. Expectations for recovery must be realistic. These syndromes require a specialized care approach.
Medication-Induced Movement Disorders
Certain neuroleptic drugs cause secondary motor issues. They block dopamine receptors in the brain. This mimics the symptoms of Parkinson’s disease.
Antipsychotics are the most common culprits. Even some anti-nausea medications can trigger this. Symptoms usually appear shortly after starting the drug. It is a reversible condition in many.
Recovery often follows drug cessation. However, it can take several months. Doctors must balance mental health with motor safety.
Metabolic and Psychogenic Factors
Wilson’s disease is a rare metabolic cause. It is especially important in pediatric cases. Copper accumulation damages the basal ganglia directly. Early intervention can prevent permanent brain injury.
Hypokinesia is frequently linked to specific genetic mutations and metabolic failures, including:
- Wilson’s disease (copper metabolism)
- Danon disease and Gaucher disease
- Mitochondrial complex deficiencies (Types 1, 2, and IV)
- Autosomal recessive Parkinson types (Juvenile and Type 2)
- Kufor-Rakeb syndrome
Psychogenic movement disorders are also possible. They often appear suddenly after stress. Observation reveals inconsistent patterns during physical exams.
Aversive stimuli can sometimes trigger movement. This paradoxical effect is a diagnostic clue. It helps distinguish organic from functional causes.
Therapeutic Interventions and Management Options
Managing hypokinesia requires a multi-pronged strategy that combines medical science with practical daily adjustments.
Pharmacological and Surgical Treatments
Levodopa remains the gold standard treatment. It replaces missing dopamine in the brain. Dopamine agonists are also frequently used.
Deep Brain Stimulation is a surgical option. It uses electrodes to regulate brain activity. This can dramatically improve motor control for some. It is usually reserved for advanced cases.
| Intervention | Primary Target | Main Benefit | Typical Stage |
|---|---|---|---|
| Levodopa | Chemical balance | Mobility | Early to Advanced |
| DBS | Neural regulation | Motor control | Advanced |
| Physical Therapy | Mobility | Safety | All Stages |
| Environment Mods | Safety | Fall prevention | All Stages |
Non-Pharmacological and Physical Therapies
Dance therapy improves rhythm and balance. It uses music to bypass damaged circuits. Patients often move better while dancing.
- Specific physical therapy exercises focus on improving gait and step length.
- External cueing techniques are used to trigger movement and bypass internal blocks.
- Occupational therapy helps maintain daily independence through task adaptation.
External stimuli help bypass basal ganglia dysfunction. Using a cueing strategy is vital to overcome freezing. These sensory triggers engage alternative motor pathways.
Practical Strategies for Daily Living
Environmental adaptations are essential for safety. Remove rugs to reduce trip hazards. Install grab bars in the bathroom. These small changes prevent serious injuries at home.

Compensatory strategies help. Use velcro instead of difficult buttons. Weighted utensils can help during meals too.
Managing motor fluctuations is a daily task. Timing medication with activity is key. Keep a diary to track symptoms.
Prognosis and Complicating Lifestyle Factors
The long-term outlook for someone with hypokinesia depends heavily on the cause and their lifestyle choices.
Reversibility and Curative Perspectives
Full cures for neurodegenerative hypokinesia don’t exist yet. Management focuses on symptom control. We aim to slow the progression.
Drug-induced cases offer a better outlook. Removing the offending medication often works. The brain can recover its function.
Long-term prognosis varies by cause. Early detection remains the best tool.
| Condition Type | Reversibility Status |
|---|---|
| Drug-induced hypokinesia | High (often reversible upon cessation) |
| Post-coronary bypass (ventricular) | Possible (anterior wall improvement) |
| Neurodegenerative (Parkinson’s) | Low (focus on symptom management) |
Influence of Stress on Motor Symptoms
Emotional stress exacerbates physical rigidity quickly. Anxiety triggers a surge in inhibitory signals. This makes movement even more difficult. Many patients notice tremors worsening under pressure.
Relaxation techniques can mitigate these flare-ups. Deep breathing helps calm the nervous system.
Stress management is a medical necessity. It is not just about comfort.
Use relaxation techniques and deep breathing to mitigate rigidity and tremors exacerbated by emotional stress.
Cognitive Impairment and Motor Links
Motor decline often correlates with cognitive changes. The brain pathways for thinking and moving overlap. This creates a dual challenge.
A holistic approach is needed for advanced stages. Mental processing speed often slows down too. This is not just “aging” but disease. Caregivers must adapt to both changes.

Physical exercise supports brain health. It helps maintain cognitive function longer.
Managing reduced movement amplitude requires early detection of neurological or cardiac dysfunction to preserve motor independence. By combining pharmacological treatments with environmental adaptations and physical therapy, you can significantly improve your daily mobility. Proactive management today ensures a more fluid and stable physical future.